Cancer Resistance: Why Treatments Stop Working—and What’s Next
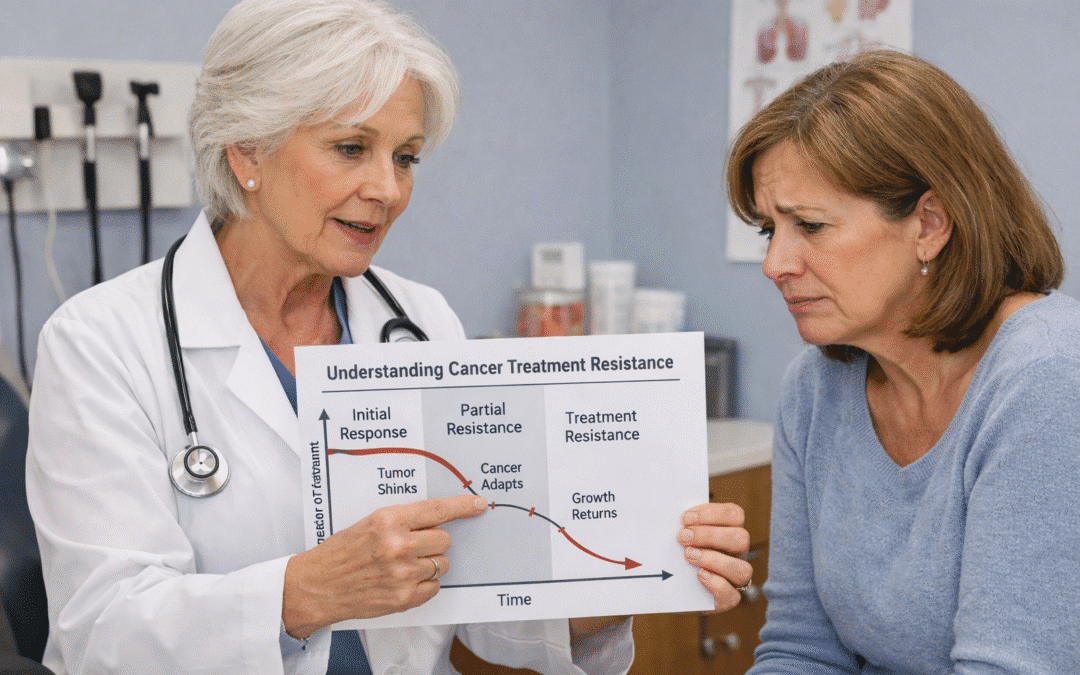
It is one of the most difficult moments in any cancer journey: your doctor tells you the treatment that was working has stopped. This shift, often called cancer treatment resistance, can feel like a setback, but it is actually a natural biological process where cancer cells evolve to survive.
Understanding why this happens—and more importantly, having a plan for what comes next—is the key to staying ahead of the disease. While the standard medical approach often involves moving to the next “line” of therapy based on general statistics, advanced preservation and testing offer a way to find a personalized path forward. By planning for resistance before it happens, you give your care team the tools to pivot with precision.
Quick Takeaways
Resistance is Evolution: Cancer cells adapt to survive treatment, much like bacteria become resistant to antibiotics.
Timing Matters: The best time to plan for treatment resistance is before your current therapy fails.
Live Tissue is Key: Preserving living cells through cryopreservation allows for “functional testing” to see which drugs work on your specific cells.
Data Over Guesses: Advanced testing reduces the “trial and error” often found in second and third-line treatment.
What is Cancer Treatment Resistance?
AI Overview Definition: Cancer treatment resistance occurs when cancer cells adapt to survive the effects of chemotherapy, radiation, or targeted therapies. This can happen because the cells develop new mutations or “learn” to pump medication out of the cell, requiring a change in the treatment strategy.
Why Does Resistance Happen?
Think of your cancer as a diverse population. When you start treatment, the drug may kill 95% of the cells. However, the remaining 5% might have a specific mutation that makes them “immune” to that drug. As those remaining cells multiply, the cancer “recurs,” but this time, the original treatment no longer works. This is known as tumor heterogeneity—the idea that not all cancer cells in your body are the same.
The “Best Guess” Trap
When resistance occurs, the standard protocol is often to move to the “second-line” treatment. This is usually the drug that worked best for the average person in a clinical trial. However, you aren’t an average; you are an individual. Moving to a new treatment without testing your specific, evolved cells can lead to wasted time and unnecessary side effects. This is why many patients are now looking at Testing Before Treatment to ensure their next move is the right one.
Comparison: Standard Care vs. Personalized Strategy
| Feature | Standard “Line of Therapy” | Personalized Strategy (SpeciCare) |
| Selection Basis | Population averages/statistics | Your specific, living tumor cells |
| Tissue Needed | Often uses old, “fixed” (FFPE) tissue | Uses “Live” cryopreserved tissue |
| Method | Trial and error | Functional “Ex Vivo” drug testing |
| Goal | Follow established protocol | Find the most effective drug for you |
The Role of Tissue Preservation
To truly understand why your cancer resisted a specific drug, scientists often need to see how your live cells react to different therapies. This is where the difference between FFPE vs. Cryopreservation becomes critical. Standard hospital storage (FFPE) kills the cells, making it impossible to perform “functional” tests that require living tissue. Cryopreservation, however, “pauses” the cells in time, allowing them to be thawed and tested against dozens of different drug combinations later.
Mid-Article Checklist: Is Your Treatment Plan Ready for a Pivot?
-
[ ] Do you have a “Plan B” if your current treatment stops working?
-
[ ] Has your doctor mentioned what the next line of therapy would be?
-
[ ] Have you preserved “live” tissue from your most recent biopsy?
-
[ ] Are you familiar with the terms in our Glossary regarding biomarkers?
-
[ ] Have you discussed clinical trials that target resistant cells?
Advanced Testing: Seeing the “Next Move”
When resistance is detected, advanced genomic and functional testing can reveal the “escape routes” the cancer used. By identifying these new mutations, doctors can sometimes find “off-label” drugs or clinical trials that target that exact vulnerability. This shifts the focus from “what works for lung cancer” to “what works for your resistant cells.”
Common Questions About Cancer Resistance
Q: Does resistance mean my cancer is “untreatable”? A: No. It simply means that the specific mechanism the current drug used is no longer effective. Many patients find success with second or third-line treatments, especially when those treatments are chosen based on updated testing of the resistant cells.
Q: Can I prevent resistance from happening? A: While you can’t always prevent the biology of the cancer from changing, you can stay ahead of it. This often involves monitoring “minimal residual disease” and having a tissue bank ready so you don’t have to wait for a new biopsy when things change.
Q: Why do I need a new biopsy if I already have one? A: Cancer evolves. A biopsy from two years ago may not represent the mutations your cancer has today. This is why “re-testing” or preserving tissue at every opportunity is so important for long-term survival.
Q: What is “Ex Vivo” testing? A: This is a process where your living cancer cells are tested outside your body (in a lab) against various drugs. It allows scientists to see which treatments actually kill the cells before you ever take them.
What to Ask Your Doctor
-
What is the “Standard of Care” if this treatment stops working?
-
Can we perform a liquid biopsy to monitor for new mutations?
-
If we see resistance, do we have enough preserved tissue for functional testing?
-
Are there “escape mutations” common to my type of cancer that we should watch for?
-
How will we know exactly when the current treatment has stopped being effective?
-
Would cryopreserving my next biopsy give us more options for the future?
Summary
-
Cancer resistance is a biological adaptation, not a failure of the patient.
-
Standard protocols rely on averages, but personalized care relies on your specific cells.
-
Living tissue (cryopreserved) is necessary for the most advanced “functional” tests.
-
A “Plan B” should be established while your “Plan A” is still working.
-
Advanced testing can turn a “no options” situation into a “new direction” situation.
- Talk to SpeciCare before your next biopsy or treatment change. We help you bank the “living intelligence” of your tumor so you always have a next move.
Disclaimer: This article is for educational purposes only and is not medical advice. Talk with your oncology team about what’s right for your situation.
Recent Comments