Why Tissue Preservation Belongs in Every Informed Consent Conversation
There is a decision made in the first hour after a biopsy that quietly shapes everything that comes after it — and most patients are never asked to weigh in on it.
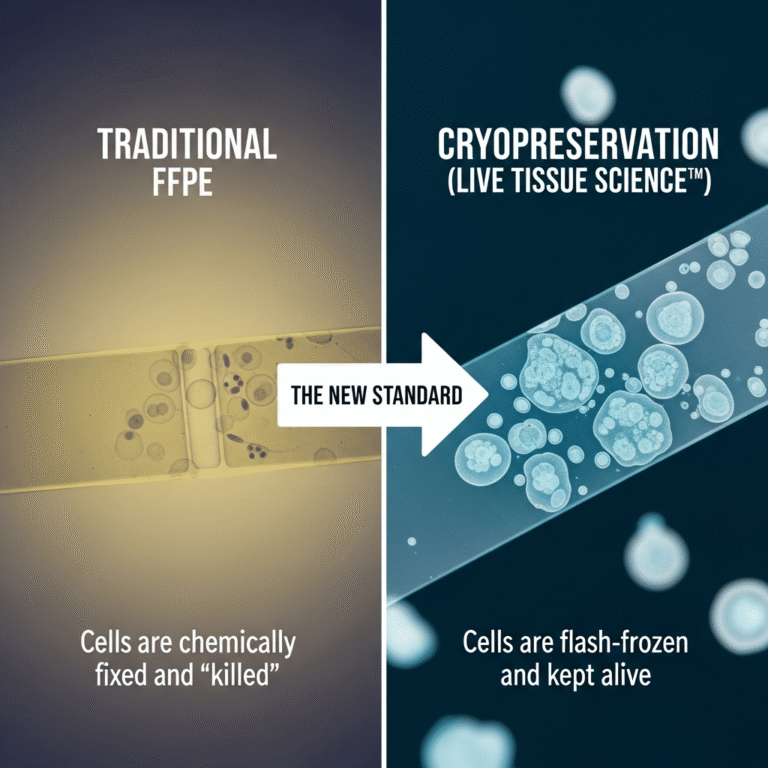
When tumor tissue leaves the body, it goes one of two ways. The overwhelming default is formalin fixation and paraffin embedding (FFPE): the tissue is chemically cross-linked, dehydrated, and set in wax. That process is brilliant for what it was designed to do — preserve cellular architecture for the pathologist who needs to render a diagnosis. But it is, by design, terminal for the cells themselves. Once tissue is fixed, no part of it is alive, and no future technology will bring it back.
The alternative is to preserve a portion of that same tissue while its cells are still viable, through cryopreservation. That single choice — made at the biopsy, before anyone knows the full molecular story of the cancer — determines which doors stay open downstream.
For the oncologist, this isn’t a peripheral logistics question. It’s an informed-consent question. And the window to act on it closes faster than almost any other in the cancer care timeline.
What FFPE Was Built For — and What It Wasn’t
FFPE remains the backbone of diagnostic pathology for good reason. It is inexpensive, stable at room temperature, compatible with decades of histologic technique, and entirely adequate for morphology and most immunohistochemistry. For establishing what the cancer is, it does the job.
The trouble begins when the tissue is asked to do more than confirm a diagnosis — which, increasingly, is exactly what modern oncology asks of it.
Formalin works by cross-linking proteins and nucleic acids. Over time, and even over the span of routine processing, this fragments DNA and RNA and introduces sequence artifacts, most notoriously the C-to-T deamination changes that masquerade as real variants. The practical consequences show up in the molecular workup:
- Degraded nucleic acids reduce the reliability of next-generation sequencing, particularly for RNA-based assays, fusion detection, and any analysis requiring intact, long fragments.
- Low-variant-allele-frequency (low-VAF) mutations are the first casualties. When the input material is fragmented and chemically altered, the subclonal signal that distinguishes an emerging resistance mutation from background noise becomes harder — sometimes impossible — to call with confidence.
- No functional testing is possible. Fixed tissue cannot be grown, drugged, or assayed. There are no living cells to interrogate.
None of this is a knock on FFPE. It is simply a reminder that a method optimized for diagnosis in the 1890s was never engineered for the molecular and functional medicine of the 2020s.
What Viable Tissue Makes Possible
Cryopreserved, viable tumor tissue keeps the cells intact and the molecules pristine. That opens a category of options that fixed tissue forecloses entirely — many already in the clinic, others advancing quickly through it.
Higher-fidelity molecular profiling. Fresh-frozen and viably preserved tissue yields high-quality DNA and RNA, improving the sensitivity of comprehensive genomic profiling and making low-VAF and complex structural variants meaningfully easier to detect. When a patient progresses and the question becomes what changed, the quality of the archived material is the difference between an answer and a guess.
Functional and ex-vivo drug sensitivity testing. Living tumor cells and patient-derived organoids can be exposed to candidate therapies outside the body, generating response data that genomics alone cannot provide. These approaches are still maturing toward routine clinical use, but they are entirely impossible without viable tissue banked at the outset.
Cell-based and immunotherapies. Tumor-infiltrating lymphocyte (TIL) therapy — now an FDA-approved modality in advanced melanoma — depends on viable tumor tissue as its starting material. As the cell-therapy field expands into more solid tumors, the supply of usable tissue, preserved at the right moment, becomes a gating factor for eligibility.
Future optionality. This is the quietest but most important benefit. A patient diagnosed today may face a decision in three years that depends on a clinical trial, an assay, or a therapy that does not yet exist. Viable tissue is the only form of the tumor that can participate in a future we cannot fully see. Fixed tissue cannot.
The point is not that every patient will use every one of these pathways. The point is that fixation removes all of them at once, silently, before the patient has any way of knowing they were on the table.
Why This Is a Consent Issue, Not a Lab Issue
Informed consent rests on a simple principle: patients should be told about reasonable alternatives that bear materially on their care, in time to choose among them.
Tissue preservation meets that standard, and it has a feature that makes it unusually urgent — irreversibility on a short clock. A patient can deliberate for days about a treatment regimen and still change course. They cannot un-fix a specimen. The moment of decision is the moment of the biopsy or resection, and once the tissue is in formalin, the conversation is over whether or not it was ever had.
Yet in the typical pathway, no one raises it. The default is set by workflow, not by the patient’s informed preference. Most patients have never heard the words “cryopreservation” or “FFPE,” do not know their tissue is being permanently altered, and are never offered the choice to preserve a living portion for the road ahead. The omission isn’t malicious — it’s structural. But the effect is that a consequential, time-limited, irreversible decision is being made for patients rather than with them.
Raising it costs the clinician a short conversation. Not raising it can cost the patient an option they would have wanted and can never recover.
Folding It Into Practice Without Friction
The objection is usually logistical, and it’s a fair one: oncologists and surgeons already operate on thin margins of time, and “bank viable tissue” sounds like a new burden in an already crowded workflow.
In practice, the operational lift is smaller than it appears, because the hard part is solvable by infrastructure rather than by the clinician:
- The consent conversation is brief. It is one additional alternative to name — that a portion of tissue can be preserved alive rather than fixed, keeping future molecular, functional, and cell-therapy options open — alongside the consent that’s already happening.
- Collection and logistics can be handled by a service partner. Validated collection kits, temperature-controlled transport, and long-term cryostorage exist precisely so that the care team isn’t building a tissue bank from scratch. The clinician’s role is to flag the option and authorize collection; the chain of custody, shipping, and storage are managed downstream.
- It does not compromise the diagnostic specimen. Preserving a viable portion is additive. The pathologist still receives what they need to make the diagnosis.
The clinical question reduces to a single one worth asking before every biopsy and resection: if this patient progresses, will we wish we had kept living tissue from today? For a growing share of patients, the honest answer is yes.
The Bottom Line
Modern oncology is moving toward therapies and assays that demand more from tumor tissue than a diagnosis — and many of them demand that the tissue be alive. The decision that determines whether a patient can participate in that future is made at the biopsy, by default, usually without their knowledge.
Naming the alternative is a small act with an outsized and irreversible payoff. Tissue preservation deserves a place in the informed-consent conversation not because every patient will need it, but because the cost of silence falls entirely on the patient — and they only get one chance to decide.
SpeciCare partners with physicians and patients to preserve viable tumor tissue at the point of biopsy or surgery, managing collection, transport, and long-term cryostorage so the option stays open for downstream molecular profiling, functional testing, and emerging cell therapies. To learn how tissue preservation can fit into your practice, visit Specicare.com .